Within two months of the day COVID-19 was first identified in Wisconsin, the state saw a sustained surge of new cases, racing past 1,200 lab-confirmed infections by the end of March 2020.
The true number of people with COVID-19 in Wisconsin is undoubtedly much higher than the official tally, and continues to climb, though no one knows by exactly how much.
“It’s fair to assume that … as high as 10 times as many people have been infected compared to what’s diagnosed,” said Dr. Ryan Westergaard, chief medical officer and state epidemiologist for communicable diseases at the Wisconsin Department of Health Services, in a media call on March 27.
This discrepancy is in part because some people have very mild infections and may not feel ill, but also because there are simply not enough resources available to test most people who are sick — in Wisconsin and across the United States. The dilemma is spurring local and regional health systems to increasingly take testing matters into their own hands, a move state officials not only endorse but are actively pursuing.
That is because even as Wisconsin has moved swiftly toward physical isolation as a means of controlling COVID-19’s spread, in terms of testing, it remains in catch-up mode along with the rest of the United States. The unknown magnitude of the difference between confirmed illnesses and the scores of infected but untested individuals — those who may be asymptomatic and unknowingly spreading the disease — makes the already challenging prospect of controlling COVID-19 nearly impossible, according to public health officials.
“You cannot fight a fire blindfolded,” said Tedros Adhanom Ghebreyesus, chief of the World Health Organization, in a March 16 briefing. “The most effective way to prevent infections and save lives is breaking the chains of transmission. And to do that, you must test and isolate.”
How the pandemic progresses in Wisconsin will depend a lot on how widely — and quickly — testing can be expanded, a need that healthcare providers have highlighted for weeks. Among them is Chris Woleske, president and CEO of Green Bay-based Bellin Health System.
“The bottom line is that without testing, we do not know how pervasive the virus is in the community,” she said.
Playing catch-up as need for testing skyrockets
Public health laboratories and private labs alike in Wisconsin have ramped up testing for COVID-19 after early missteps by federal agencies severely restricted their ability to meet testing demands. Officials at some public health labs around the nation have even accused federal partners at the Centers for Disease Control and Prevention and Food and Drug Administration of misleading them about serious problems with the early COVID-19 test kits and testing strategy devised and approved by the agencies.
The bungled rollout has become a flashpoint in a simmering row between states and the federal government over the latter’s response to the pandemic, which a growing number of state and local leaders are criticizing as sluggish, incoherent and disastrous for public health. Still, some progress is being made as labs across the nation pump out COVID-19 test results with increasing speed.
In Wisconsin, more than 17,000 tests had been conducted by March 30, with the number of new tests growing rapidly day by day from only a few hundred per day in mid-March to more than 2,000 new test results on March 28 alone.
But even as a growing group of labs in Wisconsin come online or add to their testing capacities, the number of patients who meet the CDC’s evolving criteria for testing has exploded. At the same time, ongoing shortages of critical testing supplies and ingredients continue to hamper efforts to meet the skyrocketing demand.
All of this means that, for the near future at least, most Wisconsinites with common COVID-19 symptoms — a fever, dry cough, perhaps shortness of breath — will go untested unless they live or work in a long-term care facility, are frontline healthcare workers or are hospitalized with serious illness. Such a severe limitation on the availability of testing for a widely circulating infectious disease is unheard of in recent U.S. history.
“I can’t think of any other example in my career where the diagnostic test is just not available [to most patients],” said Dr. Michael Landrum, an infectious disease specialist at Bellin Hospital in Green Bay, in an interview on March 19.
At the time, Bellin was sending specimens taken from possible COVID-19 patients to the Wisconsin State Laboratory of Hygiene in Madison for testing. The state lab is one of two public health labs in Wisconsin, in addition to a couple of private labs, where almost all specimens went for COVID-19 analysis in the initial days and weeks after the CDC relinquished total control over testing in February.
Initially, those labs were only able to provide results for 100 or so tests per day, leaving many doctors and patients waiting for results for up to a week. That capacity expanded significantly in the second half of March, according to Dr. Allen Bateman, assistant director of communicable diseases at the state hygiene lab. At month’s end, that laboratory was able to run about 400 tests per day, while the Milwaukee Health Department could run an additional 100-150 tests.
Much of that expanded capacity is a result of simply maximizing the hours that lab technicians are pushing tests through. The state hygiene lab abandoned its normal operating hours and moved to nearly constant testing: 7 days per week, with the only breaks being in the overnight hours.
But even with expanded hours, there are limits to the state lab’s capacity. These constraints are primarily related to an extremely crunched supply of the tools and ingredients needed to conduct a COVID-19 test. The shortages are key to understanding why testing for COVID-19 remains unavailable to most people in Wisconsin, including those with mild or moderate symptoms.
“We theoretically could test more than 400 for a day or two,” Bateman said. “But then we would no longer have any supplies to test any of those high-priority patients two days from now.”
But if Wisconsin and the U.S. are to get a firmer handle on the outbreak, experts argue testing must expand well beyond high-priority patients. That’s been a successful strategy in some nations that have managed to slow the pace of their outbreaks, at least for the time being, including South Korea, Singapore and Taiwan.
Private health systems go their own way
With the public health system hamstrung by supply shortages, some private health systems and commercial lab suppliers have tried to meet demand by developing their own COVID-19 tests. Only systems with major research labs have the capability to do so. In Wisconsin, these include the Froedtert health system headquartered in Milwaukee, La Crosse-based Gundersen Health System, the University Hospital in Madison and Mayo Clinic, which is based in Rochester, Minnesota, but has many satellite hospitals and clinics in western Wisconsin.
Gundersen’s COVID-19 test was developed with assistance from the University of Wisconsin-La Crosse, according to Steven Calliseter, a microbiologist at the health system’s research laboratory. Gundersen was motivated to make its own test so its patients could be more quickly informed about their infection status, Callister said in a March 27 segment on PBS Wisconsin’s Here & Now.
“That’s going to be the key to slowing down this virus,” he said. “You need to identify the people that have it.”
Mayo also operates a hospital and satellite clinics in the La Crosse area, along with sites throughout west and northwest Wisconsin. The clinic began developing its own COVID-19 test within a week of a Feb. 4 federal declaration that opened the door to private labs seeking to make an alternative to the test developed and controlled by the CDC. Mayo began developing its test a week later.
“We started diligently working at really an unprecedented pace to develop and implement the test,” said Dr. Bobbi Pritt, a microbiologist at Mayo who coordinates its laboratory response to disease outbreaks.
A significant factor in the limited availability of tests, at least initially, was the simple fact that the virus that causes COVID-19 — called SARS-CoV-2 — is brand new to humans. Any diagnostic tests that detect the virus and consequently confirm an infection are therefore by definition also brand new and must be cobbled together from scratch.
Luckily for labs like Mayo’s, similar tests had been developed to detect SARS-CoV-2’s genetic cousin, the original SARS virus. Additionally, the CDC published a guide to performing its test for the new virus, and that offered a useful framework to follow.
Pritt compared the process to developing a recipe, say for a cake, except in this case the product is not a luscious confection but rather the ability to reliably detect a portion of the genetic fingerprint of the SARS-CoV-2 virus within a sample of human cells retrieved from a patient’s nasopharynx.
“When you do that, you pick a [genetic] target that is part of the virus’s core structure,” Pritt said.
Ideally, this target is a portion of the virus’s genetic material that is very stable and not likely to mutate, such as a portion required for the virus’s self-assembly. Once the target is selected, a series of experiments help determine the steps, tools and materials needed to reliably identify the genetic material when it is present in a specimen.
“Very much like when you bake a cake, when you may decide that you need a little more flour or a little more milk, so you have to keep tweaking the components,” Pritt said. “There are several different components that go into making a test like this, so it’s a lot of trial and error. Usually it takes months of doing experiments to really determine what the best combination is to make the tastiest cake, so to speak.”
In this case, thanks to ceaseless experimentation, Mayo completed its test on March 11, exactly one month after setting out.
“We had people working around the clock,” Pritt said. “Coming in on weekends, coming in at 5 in the morning, working till midnight to develop and then validate this test.”
Deploying tests in the field
Mayo’s new test went into use March 12, first only to patients at its Rochester campus, but soon to patients across Mayo’s network of clinics in Minnesota, Iowa and Wisconsin, and eventually to patients outside of its network.
“We’ve been steadily expanding and expanding and expanding,” said Dr. Bobbi Pritt said.
Mayo Clinic can now process upward of 800 specimens a day using its own test and has added capacity for up to 4,000 additional tests per day after purchasing a new test from a commercial manufacturer that developed its own test kit through a similar recipe-building process. Mayo plans to add a second commercial test kit that would expand capacity by another 1,200 tests each day.
Crucially, the commercial test kits come pre-assembled — reducing the labor involved at the Mayo labs — and can be run through different instruments than Mayo’s home-baked tests. In addition to a shortage of supplies and ingredients, another bottleneck in many labs, including Mayo and the state hygiene lab, has been the capacity of specialized instruments needed to perform the tests.
Still, the primary shortages affecting all labs, whether they are using a privately-developed test, a commercial test or the public CDC test, are in basic materials.
“The manufacturers are running into the same problems we are, where they might run out of components and not be able to produce the test fast enough,” Pritt said.
At the same time, Wisconsin officials have fielded anecdotal reports that some testing supplies are being diverted to parts of the U.S. where outbreaks are quickly accelerating into full-blown crises, such as in New York.
“We are hearing reports from our lab partners around the state that there is some diversion happening,” said Wisconsin Department of Health Services Secretary-designee Andrea Palm. “[Labs] are hearing from their suppliers that they are moving product to other states,” Palm said. “And so we have expressed concern to our partners at the federal government about that diversion.”
Dealing with a shortage of ‘everything’
A recurring theme of the COVID-19 outbreak in the U.S. is the shortage of almost every human and material resource needed to combat it. These shortages affect almost every aspect of testing.
“Everything is in short supply,” said Mayo Clinic’s Dr. Bobbi Pritt.
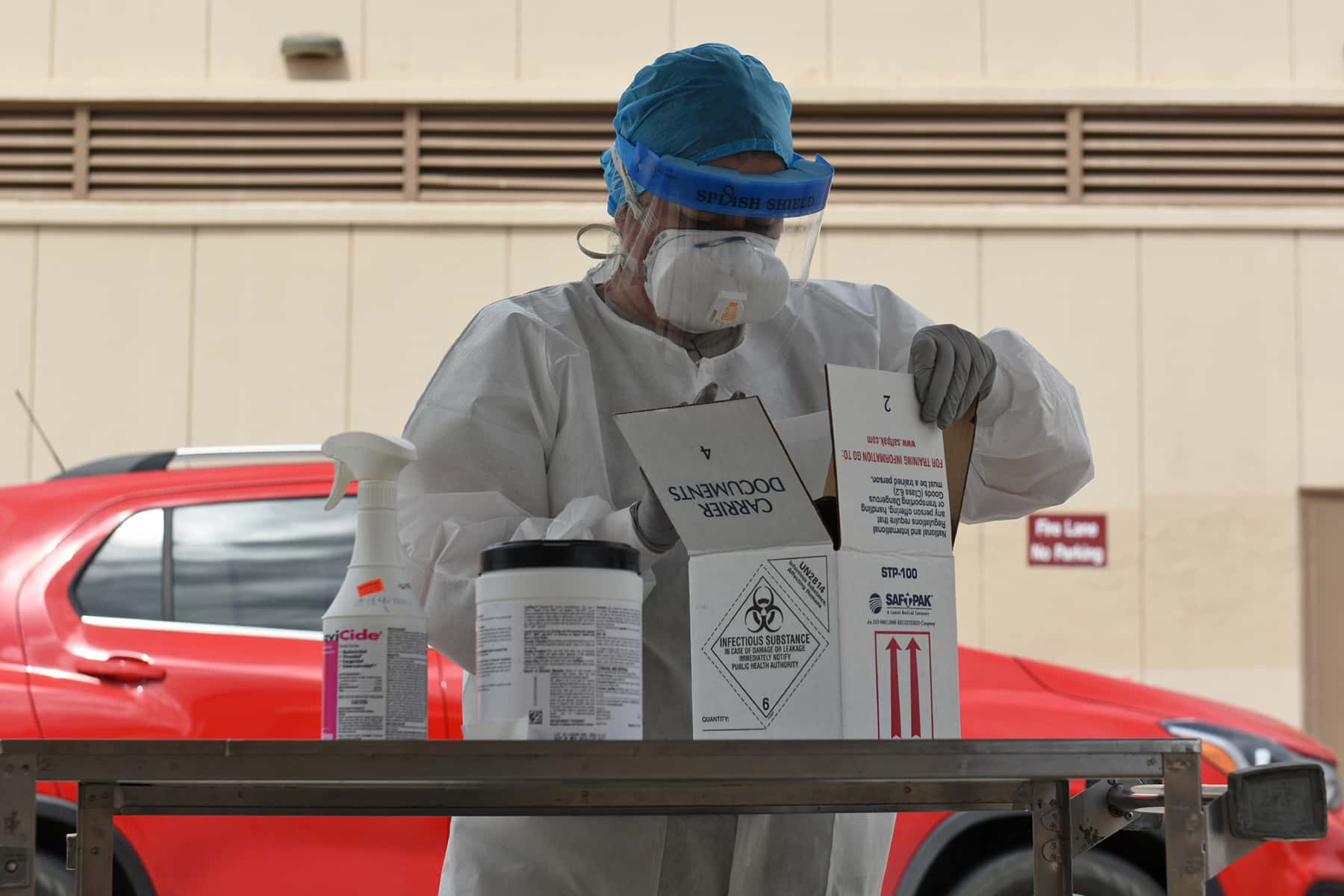
There aren’t enough nasopharyngeal swabs — the long, flexible, specialized instruments required for taking a specimen from a hard-to-reach part of a patient’s upper respiratory system. Only a few manufacturers make these swabs, including a key supplier located in northern Italy, a region crippled by the virus.
Additionally, specimen collection is uncomfortable for patients and often leads to coughing or sneezing fits, so healthcare workers performing the collection must be geared up with face shields, gloves and other personal protective equipment. That equipment is also scarce.
There is the liquid needed to maintain specimens as they await testing. Called viral transport media, it is also in severely short supply, and the CDC has urged labs to create their own if possible. The FDA has approved a substitute for viral transport media — neutral saline. The approval may help alleviate some pressure on the transport media’s supply.
Then there are the ingredients needed to prepare and analyze specimens at the lab in a process called polymerase chain reaction, or PCR. In the case of COVID-19 testing, PCR is used to detect and amplify the targeted bit of the SARS-CoV-2 virus’s genetic material that scientists know to be highly stable.
The ingredients needed for this process are called reagents. They kickstart chemical reactions that perform various functions — from extracting and amplifying the virus’s genetic material to binding to that material and emitting an unmistakable fluorescent signal. Labs have had trouble maintaining a supply of these reagents, particularly the ones that set off the chemical reaction that extracts the viral genetic material from a specimen.
“The reagents for that are really limited right now,” said Dr. Allen Bateman of the state hygiene lab.
Meanwhile, as a growing number of private health systems attempt to work around the public health system’s limitations by developing their own tests or purchasing test kits through commercial manufacturers, demand for all of these materials has only increased.
The spiking demand has manufacturers of the reagents and instruments needed to perform PCR in overdrive. Among them is Madison-based Promega, a life sciences company with manufacturing facilities in Wisconsin, California, China and South Korea. Promega manufactures several reagents needed in the PCR process. The company supplies the reagents both directly to labs and to more than a dozen commercial manufacturers of COVID-19 test kits.
“We’re seeing that ramp up tremendously,” said Chuck York, vice president of manufacturing at Promega. “Demand is exceeding what we can produce on a weekly basis.”
York said the company has production lines going at a near-constant pace, particularly for the reagents needed to extract the viral genetic material from a specimen.
“That’s our most challenging area,” he said. “That’s one of the areas we are running seven days a week, three shifts, and we’re bringing more capacity online.”
York said the company estimates it has produced reagents to support some 20 million COVID-19 tests since January.
“We’re fortunate that our staff that are on the front lines continue to be very motivated by the impact we’re having on everybody out there in the rest of the world,” he said.
Cautious optimism about testing capacity
Promega is one of several Wisconsin-based companies that have been tapped by Gov. Tony Evers’ administration to take part in a newly formed COVID-19 testing “strike team” announced in late March.
In what Evers described as a public-private partnership, the team includes a mix of Wisconsin-based technology companies and private health systems with wide name recognition in the state — Epic Systems, Exact Sciences, the Marshfield Clinic, Froedtert health system and UW Health among them.
The partnership’s immediate goals include an initial doubling of testing capacity in the state, according to Andrea Palm, the state health department secretary-designee. Still, she stopped short of promising a broad expansion of testing that would make it available to lower-risk individuals and people with mild symptoms.
“We do want to make testing a little more widely available,” Palm said during a March 30 media call announcing the effort. However, she added, “We certainly are not at a point where we would recommend testing for everyone.”
Instead, state health officials envision an eventual testing protocol for COVID-19 that mirrors testing for influenza: widely available to symptomatic patients so long as they have a doctor’s order. Meanwhile, those involved in testing for COVID-19 in Wisconsin are hopeful that supply chains can be strengthened as the outbreak progresses.
“I am cautiously optimistic,” said Dr. Bobbi Pritt, adding that Mayo Clinic has also been in touch with health officials in Wisconsin about the state’s testing needs. “I think we’re in a very strong position to continue to support Mayo. And we’re going to continue to expand capacity as possible so that we can help as many people as possible.”
Additionally, state epidemiologist Dr. Ryan Westergaard said during a March 27 interview on Wisconsin Public Radio’s The Morning Show that about 40 labs in Wisconsin were testing for COVID-19. That capacity could provide results for around 2,000 tests each day, a four-fold increase above the output just a week or two earlier. For his part, Dr. Allen Bateman of the state hygiene lab said he welcomes the entrance of more health systems into the COVID-19 testing arena.
“I think the diffuse model of having testing available in as many places as possible is the best way to go,” Bateman said. Widely available testing would reduce the pressure on large centralized operations, but it could also considerably shorten the time between when a specimen is taken and results are available.
Bateman said he is especially enthusiastic about recent FDA approval for a COVID-19 test kit developed by the manufacturer Cepheid. The test is compatible with the company’s rapid testing platform, which Bateman said is a “very common” instrument in diagnostic labs across Wisconsin and the U.S. The test promises results in as little as 45 minutes, light-years faster than the state’s current turnaround time of 1-2 days, plus the time of transit.
Another test developed by lab supply manufacturer Abbott would cut down the time to results to just 5 minutes for labs with the proper instruments.
“We are in a much better place than we were a week or two ago,” Bateman said.
Whether the position of Wisconsin’s diagnostic labs continues to improve will largely depend on whether the supply of reagents, swabs, protective equipment and instrumentation can rise with demand.
“I think all hospitals are looking to try to bring [testing] online,” said Dr. Michael Landrum of Bellin. “It’s just the limitation of the supplies.”


Will Cushman
United States Department of Defense
Originally published on WisContext.org, which produced the article in a partnership between Wisconsin Public Radio, Wisconsin Public Television and Cooperative Extension.